|
Upper extremity casts
Casts on the upper extremity may extend
above the elbow or be limited to the forearm and hand. In either case,
the cast should be trimmed along the line of the knuckles on the dorsum
and obliquely across the proximal flexion crease of the palm on the
volar side to allow unrestricted motion of the fingers.
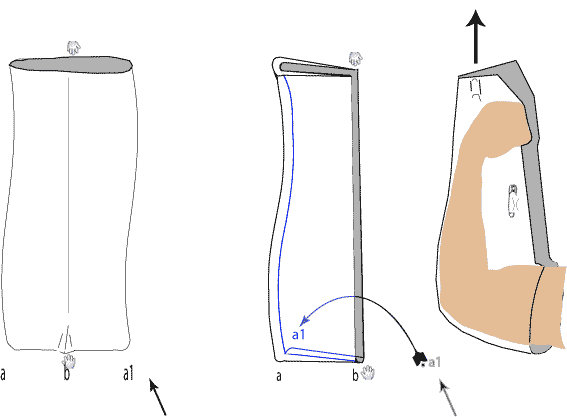
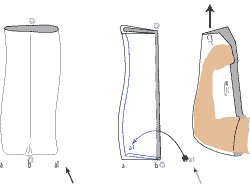
Three points of contact should be mould ed into the cast. These points
reverse the direction of displacement and hold the
fracture fragments reduced. A contact point should not cross a joint.
Take care to ensure these contact points are smooth, make them wide,
and gradual, with the base of your thumb or plam.Th ese points should
not cause discomfort to your patient.
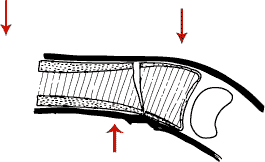 |
| Three points of contact should be mould ed into
a plaster |
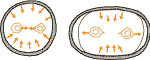 |
| Make the cross-section of your forearm cast oval.
Otherwise falling in may result in possible cross union |
A hole should be cut out around the thumb
just large enough to allow unrestricted motion. – This means
that the distal end of the cast should extend to the level of the
MP joints The edges of this thumb hole must be carefully everted,
so that the sharp edge does not cut the skin. Occasionally, the thumb
may be included in the cast, as in treating scaphoid fractures.
 |
| Pillow slip method of elevating upper limb. Turn
the slip half inside out,along its length as shown. Use this sling
to suspend the upper limb vertically from a drip stand, so that
the fracture is just above the level of the heart. |
Post manipulation immobilisation: If the patient has to lie in bed the pillow
slip method of elevation can be used.
Lower-Extremity Casts
.
 |
The first plaster is best applied with the knee bent 90
degrees over the end of the table. Traction is then applied by
an assistant, (or a bucket of water as depicted here) Make sure
the rotation, as well as the alignment is corrected. Velband
is then applied, and the pop applied to the lower leg.
The knee is then straightened to 15 degrees, and the above knee
POP completed. |
Long-leg casts may be applied with
the knee flexed or extended, but if weight-bearing is to be allowed,
the knee should be neutral or in 5° of flexion.
 |
| Application of padding |

|
BK Pop
Take up slack
by making tucks in the plaster bandage |
The cast should be trimmed in line with the metatarsal heads on the
plantar aspect and at the base of the toes dorsally. The fifth toe must
be entirely free; this is a common site for a plaster sore. Perkins
stated that it is most important not to immobilize the forefoot in varus,
and he left the metatarsal heads free to bear weight. If a toe plate
is used, the metatarsophalangeal joints must not be held in hyperextension.
In fractures of the lower third of the tibia, dorsiflexion of the foot
frequently causes angulation of the fracture. It is quite permissible
under these circumstances to immobilize the foot in plantar flexion,
although in fractures of the ankle this would be proscribed. When the
foot is immobilized in plantar flexion and a walking heel is applied,
the contra lateral shoe should be raised to equalize leg lengths.
Many orthopaedic surgeons reinforce
their casts by applying splints to the posterior aspect of the cast.
This adds weight without adding much strength. The same amount of
plaster applied anteriorly as a fin strengthens the cast
immeasurably, making fracture of the cast at the ankle virtually
impossible
Points in applying above knee cast
-
Proximal end – as high in the
groin as possible
Distal end – To MP joints of
foot
Knee in 5 to 15 degrees flexion
Foot in at 90 degrees to tibia
Hip and Shoulder Spicas
Avoid the use of hip and shoulder spicas
in adults. They are more readily tolerated in children. Make sure
there is someone at home during the day to care for the patient you
discharge in a spica. In the past, patients were frequently sent home
in hip spicas to make space in hospitals. In their home environment,
if no one cares for them, they may lie unturned, soaking in their
own urine and feces and manufacturing immense decubitus ulcers. We
have seen a paraplegic woman with a fractured spine transported in
a double hip spica, who on arrival had bone showing over both iliac
spines, both greater trochanters, and her sacrum
 |
| Spica Cast
A one and a half spica cast.
The leg portions are reinforced with a piece of wood. Beware also
of "registrar's" corner - the portion behind the buttocks
often neglected and this can cause breakage |
It is hazardous to place patients in spicas when they lack sensation,
and it is only under the most unusual circumstances that we would now
advocate the use of the hip spica in adult fractures; however, they
may still play a role in children's' fractures.
To reduce the weight of these casts
and make the patient more comfortable, a substantial window should be
cut out over the belly. This portion of the cast contributes nothing
to its strength, but the window should always be circular or oval and
never rectangular, because corners act as stress risers. This means
that it is best cut with a knife. If one waits too long, cutting the
hard plaster can be tedious. The task is made easier by outlining the
window with the knife and then making a cross with the plaster saw
within the circle. The free corners may then be pried up and the
cutting of the circumference completed with
Older orthopaedic surgeons at some time
or other in their career have been embarrassed by the disconcerting
habit that spicas have of breaking at the hip. This is sometimes
caused when a triangular area, commonly known as the "amateur's corner," at the junction of the limb and trunk does not receive
its fair share of the plaster. It also results, as Strange pointed
out, from the juncture of the body and leg being an open section and
thus very much weaker than the circular portions of the cast. To strengthen this weak point, fin-like reinforcements are
applied anteriorly, posteriorly, and laterally, much in the same way
that a walking cast might be reinforced apply a new cast.
|
|