|
Operative choices When operations are planned on the bony skeleton, the following broad categories of operations are available. Factors such as age and physical fitness are important in making the choice regarding the most appropriate procedure
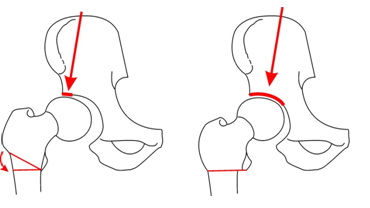
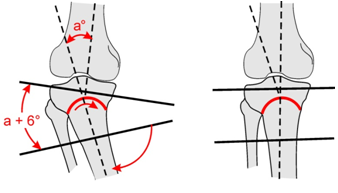
OsteotomiesAn osteotomy is the section and realignment of a bone. This realigns the bone and may be used to correct an existing deformity e.g. varus of the tibia. Realignment also redistributes the forces over a joint and a normal area of the joint can be loaded in preference to the pathological e.g. osteoarthritic areas.
Hip Osteotomy
Indications Osteotomy
Contraindications
Arthrodesis The joint is surgically fused in a position of function. Arthrodeses are usually indicated in the younger patient with mono arthritis. E.g. Posttraumatic osteoarthritis of the hip in a 20 year old active patient.Indications Arthrodesis
Contraindications hip Arthrodesis
 A hip arthrodesis would be contraindicated in avascualar
necrosis of the hip caused by alcohol or steroids as there is a high chance
the other hip will develop AVN too. A hip arthrodesis would be contraindicated in avascualar
necrosis of the hip caused by alcohol or steroids as there is a high chance
the other hip will develop AVN too.
Excision Arthroplasty The joint is excised on one or both sides. Examples are the Girdlestone arthroplasty of the hip. Here the femur head and neck are excised. A Keller's operation of the first MP Joint of the big toe was a popular operation for hallux valgus with joint degeneration. The proximal end of the first phalanx was excised.
Indications Girdlestone
Girdlestone operations are rarely done these days, but are a choice where sepsis precludes total hip replacement. They leave a mobile joint but always result in some shortening of the femur and are never entirely pain free.
Joint ReplacementJoint replacement is a cost-effective way of rehabilitating a patient with arthritis of the hip, knee and even shoulder.
Types of joint replacement
The “Gold Standard” is a cemented hip.
In the active younger patient an un cemented component may be used so
that bone stock is preserved for a later revision. At present a hip replacement
should last 15 or more years before a revision is needed.
Contraindications Total Hip
 
Hip Pain: Decisions as to type of operation An adolescent or child can be offered a osteotomy if the hip has more than 60 degrees of flexion. In severe hip osteoarthritis at this age, an arthrodesis is still a good choice. Between the ages of 30 and 55 years total hip replacements for OA are best avoided. Continue with conservative treatment if possible. An osteotomy can be considered if there is hip motion and a normal area of cartilage than can be moved into the superior weight bearing area by an osteotomy. In the active older patient a total hip replacement is the ideal treatment
for osteoarthritis. Because patients with autoimmune diseases such as
Rheumatoid arthritis have limited mobility, a total hip replacement can
be done at any age.
|