Lower Limb
Inability to dorsiflex the foot can be controlled with splints. The classical type of splint is the below knee caliper. Other types include the 0' Gorman spring and, with the advent of thermoplastics, the Ankle Foot Orthosis (AFO)
 |
 |
 |
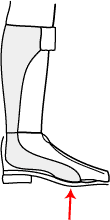 |
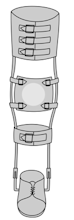
| Ischial weight bearing caliper. Used to relieve axial loading on femur. | Lace-up Caliper: Use to control limb alignment | O' Gorman Spring | Ankle foot orthosis. The elasticity of this low profile splint provides an upward force on the foot |
The decision about the type depends on how much resistance due to spasticity and other factors, there is.
- Below knee caliper with back stop - spasticity present
- Spring type - mild resistance
- Little resistance or flaccid foot - AFO type
The advantage of the AFO is that it is light, and easily tolerated by physically weak patients. It is also cosmetically much less obtrusive than the other types, as it can be hidden under clothing. If there is no spasticity, or other resisting forces, an AFO is the orthosis of choice for the drop foot.
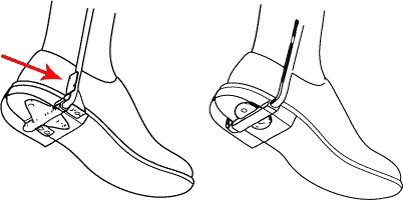 |
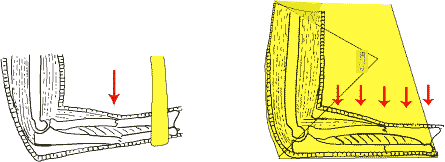
| Ankle movement control with a caliper: A backstop to the pivot of the caliper (red arrow, left) will limit plantar flexion - used for "drop" foot. A square ended pivot (right) will limit both dorsi and plantar flexion - used in a totally flail foot. |
 |
| For varus hind foot deformities, an inside iron with "T" strap is prescribed |
Upper limb splints
Fractures:
A collar and cuff is used to suspend a forearm with a cast or a humerus fracture that needs to hang under the effect of gravity. A triangular bandage is a suspension that decreases the weight of the forearm on the shoulder.
 |
| Forearm fractures: Collar and cuff (L) will cause inferior angulation, whereas a triangular bandage (R) distributes load more evenly, thus preventing sagging |
It is may be used to relieve the weight of a upper arm cast, or after shoulder trauma such as an aromio-clavicular dislocation. It is sometimes used as an alliterative to a figure of eight bandage in minimally displaced clavicular fractures.
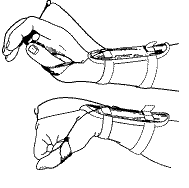 |
| A type of dynamic radial splint: The"cock up" splint |
For radial nerve paralysis the wrist has to be held in dorsi flexion. A passive dorsi flexion splint or a dynamic arrangement such as the dynamic radial extension splint (DRES splint) can be used.
Spinal Orthoses
Neck Braces
For cervical sprains and fractures a neck brace can be used. Usually unstable fractures are treated by bed rest for at least 6 weeks in traction before it is time to discharge with a brace. Even postoperative cervical fusions will require a brace on discharge from hospital.
The following are the broad indications for cervical braces.
- Soft brace - minor trauma or stable soft tissue injury
- Hard polypropylene brace . Stable soft tissue injuries.
- SOMI type braces - Cervical fractures after initial 6 weeks in traction,
postoperative cervical fusions potentially unstable soft tissue injuries.

SOMI Brace. Sterno Occipito Mental Immobiliser
Thoracolumbar
The thoracolumbar spine can also be stabilised by a variety of braces. The lumbrosacral corset is effective for the conservative treatment of lower backache.
 |
| Soft corset for lower backache |
It works on a hydraulic principle and gives rigidity to the lumbar spine in much the same way a "Rubber Duck" inflatable boat gets its rigidity from bags filled with air. It supplements weak abdominal muscles and is effective for pain control as well as in spinal stenosis where it allows easy flexion of the spine, thus opening up the posterior elements.
Hard corsets, custom made out of thermoplastics are useful in the potentially more unstable fractures of the thoraco lumbar spine.
 |
| A hard brace: Thoraco Lumbar Sacral Orthosis.(TLSO) |