Internal Rotational Deformities of the
Lower Limb
by Jason Crane
Abstract
Most rotational variations in young children, such
as in-toeing, out-toeing, and torticollis, are benign and resolve spontaneously.
Understanding the normal variations in otherwise healthy children is
vital to identifying true structural abnormalities that require intervention.
A deliberate assessment of the rotational profile is necessary when
evaluating children who in-toe or out-toe. In-toeing is usually attributable
to metatarsus adductus in the infant, internal tibial torsion in the
toddler, and femoral anteversion in children younger than 10 years.
Definition
Rotational profiles vary widely among normal children.
Differences in appearance during walking or running are most often just
that, differences and not pathological conditions. In toeing
is described by the direction of the foot, relative to the body’s
line of progression during the gait cycle. This is referred to as internal
torsion. It is produced by the summation of factors that include version
of the bones, capsular laxity or tightness and muscle control.
Natural History
Limb buds appear in the fifth week in utero. The great
toes develop in a preaxial position, rotating medially in the seventh
week to bring the hallux to midline. Subsequent intrauterine molding
causes external rotation at the hip, internal rotation of the tibia,
and variable positioning of the foot. Thus, many infants are born with
an internal tibial torsion axis, an external contracture at the hip,
or flexible foot deformities.
The external hip contracture initially masks the high
degree of femoral anteversion also characteristic of normal infants
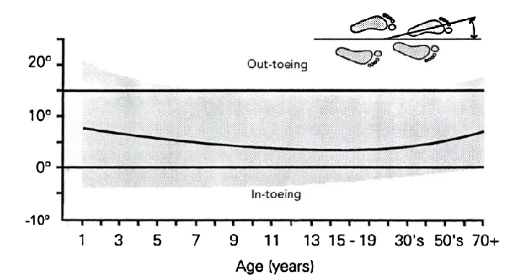
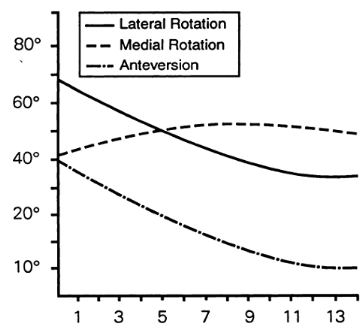
at birth. Postnatally, the lower extremities continue to rotate externally
until adult values are reached (between ages 8 and 10 years). During
this period of rapid growth, the tibia typically externally rotates
15° (-50 at birth to10o at maturity) while
femoral anteversion decreases an average of 25° (400
at birth to 15o at maturity). Normal rotational profiles
in childhood therefore are variable and age-dependent.
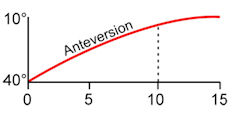
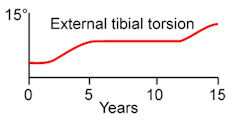
Femoral anteversion progression with age Tibial rotation progression
with age
Evaluation
Normal variability in young children must be differentiated
from more serious structural problems. The clinical history should delineate
the onset and duration of a structural problem and any evidence of progression.
Whereas the typical natural history of benign rotational conditions
would suggest improvement over time, a progressive deformity suggests
a possible pathologic developmental or neurologic disorder.
history should include a careful assessment of rotational
disorders in other family members and the presence of hereditary disorders
(eg, vitamin D–resistant rickets, mucopolysaccharidoses, achondroplasia,
epiphyseal or metaphyseal dysplasia) that may affect the rotational
profile.
The child's rotational profile, as described by Staheli,
should be recorded.
The five components in this profile are:
-
Internal and external hip rotation,
-
Thigh-foot axis,
-
Transmalleolar axis,
-
Heel-bisector angle,
-
Foot progression angle during gait.
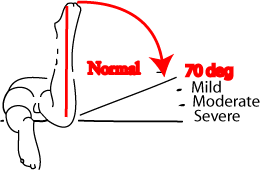
Internal and external hip rotation.
Hip rotation is most easily measured with the patient
in the prone position. Infants have an average of 40° of internal
rotation (range, 10° to 60°. The range is limited by the tight
posterior capsule even though they have increased femoral anteversion
and should potentially have a larger internal rotation arc.) and 70°
of external rotation (range, 45° to 90°). By age 10 years, internal
hip rotation averages 50° (range, 25° to 65°) and external
rotation, 45° (range, 25° to 65°). Internal rotation measuring
70°, 80°, or 90° is evidence respectively of a mild, moderate,
or severe increase in femoral torsion. Increased femoral torsion may
be evident during gait, with medially facing patellar alignment.
![[image]](internal-rotational-deformities-of-the-lower-limb/internal-rotational-deformities-of-the-lower-limb-3.png)
Thigh-foot axis
Is best examined with the child in the prone position
and the knee flexed 90°. This angle consists of the rotation of
the tibia and hindfoot in relation to the longitudinal axis of the thigh
and indicates the amount of tibial torsion present. In infants, the
thigh-foot angle averages 5° internal (range, 30° to +20°).
Excessive internal tibial torsion spontaneously resolves by age 3 or
4 years in most children. By age 8 years, the thigh-foot axis averages
10° external (range, 5° to +30°) and usually changes very
little after that.
![[image]](internal-rotational-deformities-of-the-lower-limb/internal-rotational-deformities-of-the-lower-limb-5.png)
Transmalleolar axis
Aids in determining the amount of tibial torsion present.
This axis is the angle formed at the intersection of an imaginary line
from the lateral to the medial malleolus, and a second line from the
lateral to the medial femoral condyles. At gestational age 5 months,
the fetus has approximately 20° of internal tibial torsion. The
tibia then rotates externally, and most newborns have an average of
4° of internal tibial torsion. As a child grows, the tibia continues
to rotate externally. Adults have an average of 23° of external
tibial torsion (range, 0° to 40°).
The heel-bisector angle
This is the line drawn through the midline axis of the
hindfoot and the forefoot. It is helpful in evaluating forefoot adduction
and abduction. In a neutral foot, the heel-bisector line passes through
the second web space.
Foot progression angle
The foot progression angle is the angle of the foot
relative to an imaginary straight line in the patient’s path.
Patients who in-toe are assigned a negative angular value; patients
who out-toe are given a positive value. This value represents the sum
total
effect of the child’s structural alignment (i.e.,
femoral torsion, tibial torsion, foot contour) as well as any dynamic
torsion forces resulting from muscle forces
Differential Diagnosis
In-toeing usually is caused by benign conditions such
as metatarsus adductus, excessive internal tibial torsion, and excessive
femoral torsion. Less frequently, patients have pathologic conditions
such as clubfoot, skewfoot, hip disorders, and neuromuscular diseases.
Metatarsus adductus, with or without internal tibial torsion, is the
most common cause of in-toeing from birth to 1 year. In toddlers, internal
tibial torsion causes most in-toeing. After age 3 years, in-toeing usually
is caused by increased femoral anteversion. More severe in-toeing suggests
a combination of deformities, such as internal tibial torsion and excessive
femoral anteversion.

Out-toeing typically is caused by external rotation
contracture of the hip, external tibial torsion, or external femoral
torsion. External rotation contracture of the hip capsule is a common
finding during infancy, whereas external tibial or femoral torsion is
more commonly seen in older children and adolescents who outtoe. Severe
pes planovalgus also has been associated with out-toeing. More serious
conditions, such as a slipped capital femoral epiphysis, hip dysplasia,
or coxa vara, are less common but should be considered. Severe Cerebral
palsy children may develop femoral internal rotation and tibilal external
rotation, called miserable alignment syndrome.
Treatment
Active treatment of childhood rotational disorders is
unnecessary in most cases. Treatment consists of reassurance and education
about the natural history of the condition. Bracing and shoe modifications
are unnecessary and should be actively discouraged for these normal
children.
![[image]](internal-rotational-deformities-of-the-lower-limb/internal-rotational-deformities-of-the-lower-limb-9.png)
Metatarsus Adductus
Definition
Described by Henke in 1863, metatarsus adductus is the
most common pediatric foot problem referred to orthopaedic surgeons.
It consists of medial deviation of the forefoot on the hindfoot with
a neutral or slightly valgus heel.
Incidence
Occurs in 1:5,000 live births and in 1:20 siblings of
patients with metatarsus adductus. The rate of metatarsus adductus is
higher in males, twin births, and preterm babies.
Pathogenesis
Although the exact cause of metatarsus adductus is unknown,
numerous theories exist. One is that in utero positioning causes the
deformity. Earlier studies suggested a relationship between metatarsus
adductus and hip dysplasia, but recent studies indicate no such correlation.
Clinically
Metatarsus adductus usually is seen in the first year
of life and occurs more frequently on the left side. Presenting complaints
include cosmesis, an in-toeing gait, or excessive shoe wear. On physical
examination, the foot appears C-shaped, with a concave medial border
and a convex lateral border. The hindfoot will be neutral or in valgus,
but never in varus. Range of motion of the ankle and subtalar joint
will be normal.
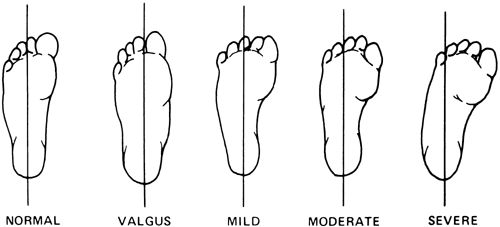
Classification
Depending on the heel-bisector angle metatarsus adductus
has been classified by Smith et al as mild, moderate, or severe. A later
classification system described by Bleck designated a flexible forefoot
as one that could be abducted beyond the midline heel bisector angle,
a partially flexible forefoot as one that could be abducted to midline,
and a rigid forefoot as one that could not be abducted to midline.
Radiology
The usefulness of radiographs before age 4 years is
limited by the lack of sufficient ossification in the bones of the foot.
In older children, forefoot adduction, excessive medial deviation at
the tarsal-metatarsal joint, and a neutral or valgus heel will be evident
on a standing radiograph.

Management
Conservative
Most cases of flexible metatarsus adductus resolve spontaneously
and do not require use of splinting, braces, or special shoes. In a
series of 21 patients (31 feet) with partly flexible or inflexible metatarsus
adductus treated with serial casting, 20 patients (95% [29 feet]) had
painless normal feet as adults Most evidence indicates that flexible
metatarsus adductus commonly resolves without treatment and that even
when it does not, it rarely leads to pain in adulthood. Patients with
rigid metatarsus adductus deformities should undergo early casting.
Surgical
Uncommonly, resistant cases of inflexible metatarsus
adductus that do not reduce with serial casting may require surgery
because of painful shoe wear. Surgery is planned between three and seven
years of age (As the midtarsal bones only ossify after 3 years of age).
Surgical options include release of the abductor hallucis tendon, medial
midfoot capsulotomy, tarsometatarsal joint capsulotomy and release of
the intermetatarsal ligaments, or osteotomy at the metatarsal bases
and cuneiforms. An opening wedge osteotomy of the medial cuneiform,
combined with a closing wedge osteotomy of the cuboid or osteotomies
at the base of the second through fourth metatarsals, has been shown
to be safe and effective. Thus, this appears to be the most effective
surgical option in patients older than 3 years with persistent rigid
metatarsus adductus deformities.
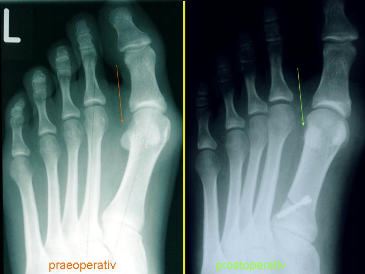
Metatarsus Primus Varus
Metatarsus primus varus is an isolated adducted first
metatarsal. In contrast with simple metatarsus adductus, in metatarsus
primus varus the lateral border of the foot has a normal alignment,
and there is often a deepened vertical skin crease on the medial border
of the foot at the tarsometatarsal joint. In general, metatarsus primus
varus is a more rigid deformity than simple metatarsus adductus, and
early casting is recommended. Persistent deformity in childhood is associated
with progressive hallux valgus. Opening medial cuneiform osteotomy has
been described for selective use in children with a severe deformity.
Dynamic Hallucis Abductus
Dynamic hallux abductus, otherwise known as the wandering
or atavistic toe, also can cause in-toeing. The great toe deviates medially
during ambulation while the remainder of the forefoot remains straight.
Dynamic hallucis abductus usually presents after a child begins walking
and is thought to be caused by an imbalance of the great toe abductor
and adductor muscles. Dynamic hallux abductus usually resolves with
age and subsequent fine motor coordination development.
Skewfoot
Skewfoot, also called congenital metatarsus varus or
serpentine metatarsus adductus, is characterized by adducted metatarsals
combined with a valgus deformity of the heel and plantarflexion of the
talus. Little is known of the pathogenesis of this disorder. Improper
casting of metatarsus adductus or clubfoot deformities may result in
a skewfoot because of failure to support the hindfoot while abducting
the forefoot in
the cast. However, most cases are thought to be idiopathic.
The amount of hindfoot valgus necessary to classify a foot as a true
skewfoot rather than as the more common metatarsus adductus is not strictly
defined.
Standing radiographs confirm the presence of an adducted
forefoot and a valgus hindfoot. The natural history of this deformity
is unclear. Although some feet undergo spontaneous correction, others
clearly continue to have pain, callosities, and problems with shoe wear.
Surgery is indicated for children with a persistently symptomatic foot
deformity.
Children are treated after age 6 years with an opening
wedge osteotomy of the calcaneus and a medial cuneiform opening osteotomy.
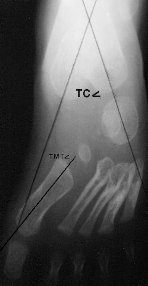
Skewfoot: An AP radiograph reveals the significant
varus deformity of the forefoot creating a negatively valued talo-first
metatarsal angle. Delayed ossification of the navicular prevents radiographic
documentation of the lateral talonavicular subluxation. The hindfoot
valgus is portrayed by the increased talocalcaneal angle (the upper
limits of normal as shown).
Tibial Torsion
Incidence
Internal tibial torsion is the most common cause of
in-toeing from ages 1 to 3 years. In two thirds of affected children,
the increased torsion is bilateral.
When unilateral, internal tibial torsion usually affects
the left side.
Pathogenesis
Most cases are thought to be caused
by intrauterine positioning.
Clinically
Accurate clinical recognition relies on measurement
of the thigh-foot and transmalleolar axes. Parents of children with
increased internal tibial torsion often report that the child is clumsy
and trips frequently.
Treatment
Conservative
Treatment with splinting, shoe modifications, exercises,
and braces has proven to be ineffective. Because the natural history
of internal tibial torsion strongly favors spontaneous resolution by
age 4 years, expectant observation is recommended instead. Disability
from persistent residual internal tibial torsion is rare, and it has
been found not to be a risk factor for degenerative joint disease. Some
have even suggested that in-toeing improves sprinting ability.
Surgical
Surgical treatment of tibial torsion is rarely indicated
and should be re- served for children older than 8 years with marked
functional or cosmetic deformity and a thigh-foot angle greater than
15°. Both proximal and supramalleolar tibial derotational osteotomies
have been used to manage tibial torsion. However, most surgeons prefer
the supramalleolar osteotomy because of its lower complication rate.
In the skeletally mature adolescent, derotational osteotomy with intramedullary
fixation is also an option.
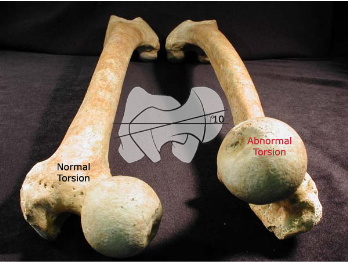
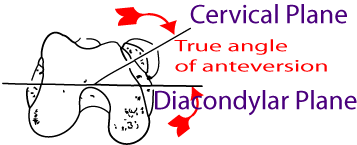
Femoral Torsion
Definition
Femoral torsion is the angular difference between the
femoral neck axis and the transcondylar axis of the knee.
Development
At birth, neonates have an average of 40° of femoral
anteversion. By age 8 years, average anteversion decreases to the typical
adult value of 15°.
Pathogenesis
Most cases of femoral torsion are idiopathic, although
a familial association is identified in some patients. No association
between increased femoral anteversion and degenerative joint disease
has been proved; however, some association with knee pain has been suggested.
Knee pain may be particularly prevalent in children with concomitantly
increased femoral anteversion and external tibial torsion (so-called
miserable malalignment syndrome).
Etiology
Increased femoral anteversion is the most common cause
of in-toeing in early childhood, tends to occur in females, and is symmetrical.
Clinically
Children with excessive femoral anteversion characteristically
sit with their legs in the W position and run with an eggbeater-type
motion (because of internal rotation of the thighs during swing phase).
In-toeing from excessive femoral anteversion usually increases until
age 5 years and then resolves by age 8.

On physical examination, internal hip rotation is increased
and external hip rotation decreased (>700 internal rotation
is classified as abnormal). Using Craig’s test; Patient
lies prone with knee flexed 900
and examiner palpates posterior aspect of greater trochanter. Hip is
then passively rotated internally and externally until greater trochanter
is parallel with examining table or reaches its most lateral prominent
position. The degree of anteversion can then be estimated, based on
the lower leg's angle with the vertical.
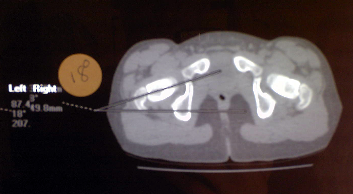
Radiology
Previously plain X-rays using the Magillian method (complicated
set of graphs and tables) were utilized to calculate the femoral anteversion.
Fluoroscopic methods using a goniometer intra procedure have also been
described. These methods have been largely replaced by CT-Scan. Cuts
are made through the femoral neck and the femoral condyles with the
patient in a static position this gives an accurate representation of
the femoral anteversion.

Treatment
Conservative
Femoral anteversion is usually self-limiting, and if
persistent causes no long term pathological changes in the associated
joints. No treatment is necessary for most cases of femoral torsion.
Surgical
Surgical intervention may be indicated in a child older
than 8 years with a marked cosmetic or functional deformity, anteversion
>50°, and internal hip rotation >80°. Surgeries to correct
femoral torsion include proximal femoral, distal femoral osteotomies
and intra medullary nails. Todd etal suggested a proximal femoral osteotomy
may be considered if the patient has a concomitant varus or valgus deformity.
Otherwise, a distal femoral osteotomy through a lateral approach is
the preferred treatment. A small compression plate may be used to treat
skeletally immature patients and a blade plate for skeletally mature
patients. This is controversial as many authors believe you should correct
proximally at the cora of the deformity. They also believe that a distal
rotational osteotomy will result in patella maltracking and patellar
femoral pain, while others maintain that you are correcting the deformity
to its normal anatomical profile and there for no maltracking should
occur.
Summary
Benign rotational variations are seen in many healthy
children. Although the physical appearance of these conditions may initially
be alarming, spontaneous resolution occurs in most cases. A thorough
understanding of the normal rotational variations that may occur in
children younger than 10 years is essential to properly reassure and
educate families, as well as to identify more serious underlying structural
problems that might exist.
References
- Common Rotational Variations in Children; Todd
L. J Am Acad Orthop Surg 2003;11:312-320
- Torsional Deformities. Schoenecker
PL; AAOS 23rd annual comprehensive review course for orthopaedic
surgeons, June 2007
- Rotational Problems in Children; Staheli
L. J Bone Joint Surg Am. 1993;75:939-949.
- Lower-extremity rotational problems in children.
Normal values to guide management. LT Staheli, J Bone Joint
Surg Am. 1985;67:39-47
|