In children the growth plate is up to five times weaker than the ligaments
stabilising the adjacent joint.The adjacent bone is also stronger than
the cartilaginous growth plate. Injury thus often leads to separation
of the growth plate leaving the ligaments and capsule intact. The separation
takes place in the middle layer (hypertrophied) of the growth plate.
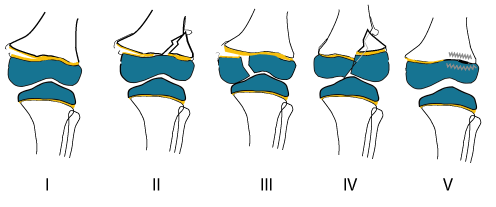
Type I Injuries Due to a separation through the growth plate of the metaphysis and diaphysis. Type II Injuries An incomplete type I with a metaphyseal bone fragment still attached to the epipyhseal end. Type I and II have a good prognosis as the blood supply to the germinal layer ( ephyseal side) is still intact and angulation and growth arrest are uncommon.
Type III Injury This fracture occurs only rarely,and is seen in the pre pubescent child. It is seen in the femur or tibia. THe mechanism is a fracture that runs completely through the epiphysis and separates part of the epiphysis and growth plate from the metaphysis. Surgery is sometimes necessary to restore the joint surface to normal. The outlook or prognosis for growth is good if the blood supply to the separated portion of the epiphysis is still intact, if the fracture is not displaced, and if a bridge of new bone has not formed at the site of the fracture. Type IV Injury Here the fracture is through the metaphysis and epiphysis. As in the type III it is intra-articular and will need open reduction and internal fixation. The prognosis for future growth disturbances and angulation is poor. Type V Injury Is due to a compression force destroying
all or part of the growth plate. This is difficult to diagnose and in
most cases is a retrospective diagnosis where angulation developed without
radiological evidence of a growth plate injury.The diagnosis can be established
with ManagementSalter Harris I and II injuries are usually managed by closed manipulation and plaster cast.
Because they are intra-articular and often displaced, types III and IV injuries require open reduction and internal fixation. Computer Tomography may help in planning the procedure. Long-Term Follow-up Long-term follow up is usually necessary to monitor the child’s recuperation and growth. Evaluation includes x rays of matching limbs at 3- to 6-month intervals for at least 2 years. Some fractures require periodic evaluations until the child’s bones have finished growing. Sometimes a growth arrest line may appear as a marker of the injury. Continued bone growth away from that line may mean that there will not be a long-term problem, and the doctor may decide to stop following the patient. PrognosisWhile most (85% of) growth plate injuries heal without complication, growth arrest and late angulation may occur .These deformities are usually minor, only 2% or less, however, prove to be significant, that is, sufficient to interfere with function 1 Factors affecting the prognosis
References (1) Shapiro F. Epiphyseal growth
plate fracture- (2) Rogers LF, Poznanski AK. Imaging of epiphyseal injuries. Radiology 1994;191:297-308.
|
Growth plate injuries
Department of Orthopaedic Surgery - Stellenbosch University
|
|