Chondrosarcoma is a cartilaginous tumour, seen mainly in the older patient. Even those tumours classified as malignant are often not fast growing. There is a wide spectrum of varying degrees of ability to metastasize. Even cartilaginous tumours, classified as benign, such as the enchondroma, have the ability to move towards the more malignant side of the spectrum. On the other hand, chondrosarcomas, classified as malignant, retain this ability to become even more aggressive, manifesting as the, so called, dedifferentiated chondrosarcoma.
Play this video screencast on chondrosarcoma management. (13 MB)
Types of Chondrosarcoma
Central chondrosarcoma.
85 % are classical central Chondrosarcoma and develop in the medullary cavity. Of the 15% developing on the surface of bone, most come from (pre-existing) osteochondromas.
The tumour is highly resistant to chemo and radiotherapy. The mainstay of treatment is surgical excision.
Mesenchymal chondrosarcoma
Has areas of cartilage and in other areas are small round cells.
Clear cell chondrosarcoma
“Empty” cells with clear cytoplasm. Commonly seen in the proximal ends of the femur and humerus.
The dedifferentiated type is at the aggressive end of the spectrum. It consists of areas of transformation into a more aggressive tumour such as osteosarcoma.
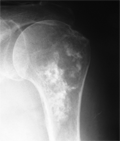
Radiological features of central chondrosarcoma
Large ill defined
Expanded
Erosion of cortex
Circular radiolucency's
Fuzzy Ca++
Soft tissue mass
Periosteal reaction
It is difficult to be certain radiologically as to the aggressiveness of this tumour. Large lesions (> 5cm) and a central location are most reliable predictors of malignancy. Punctate calcifications. Subtypes such as Mesenchymal chondrosarcoma often have more mineral is at ion than classical chondrosarcoma. If there is a moth eaten, or permeative pattern, it is probably an aggressive, high grade chondrosarcoma.
X ray of a central chondrosarcoma of the right humerus in a 60 year old. Calcification can be seen in the lesion. The lesion shows scalloping and expansion, which are signs of a more aggressive lesion.
MRI is used to determine the extent of intra osseous and soft tissue involvement.
Secondary Chondrosarcoma
Benign cartilage lesions including
Osteochondroma (<1% risk of malignant transformation)
Multiple hereditary exostosis (1-10% risk of malignant transformation)
Enchondromas (1% risk of malignant transformation)
Ollier's disease (25-40% risk of malignant transformation)
Maffucci's (100% risk of malignant transfomation)
The more lesions there are the higher the risk of malignant transformation. Suspect malignant change in a benign cartilaginous lesion that suddenly becomes painful.
Borderline cartilaginous tumours
In this group are cartilaginous tumours such as the enchondroma. It is difficult to determine histologically whether these lesions are truly benign, or are a low grade Class 1 lesion. Dahlin started the concept of the grade ½ tumour. These tumours may be treated less aggressively.
Borderline cartilage tumour, treated by curettage
X rays must be studied carefully for signs of aggressiveness. Aggressive signs include scalloping, expansion and any periosteal reaction.
Causes of pain in an osteochondroma
Soft tissue impingement
Fracture (of the neck of a pedunculated lesion)
Malignant change
On CT or MRI the cartilage cap can be measured. If >1cm wide, suspect malignancy. Do an excision biopsy of all painful osteochondromata.
The role of radio and chemotherapy
The central type needs at least 60 Gy of radiotherapy to treat. This is an large dose and is reserved for irresectable lesions.
The atypical types such as mesenchymal and clear cell, are more sensitive to radiotherapy. Chemotherapy can also be successful with these types. The dedifferentiated type may may be mor sensitive to radiotherapy.
Surgical management of central chondrosarcoma
In stage 2 and 3 lesions. Complete surgical excision is the only hope of cure.
With borderline chondrosarcoma, intra lesion al curettage, is regarded by many authors to be sufficient. Dahlin started the concept of the grade ½ tumour. It is the low grade tumour with no aggressive features, such as scalloping and cortical thinning. These are the tumours that can be managed by curettage and adjuvant. An adjuvant is an additional modality to kill tumour cells locally after he lesion has been thou roughly curetted and burred with a high seed drill. Cryosurgery or local application of phenol are commonly used for this.
The downside of this more conservative approach, is that if recurrence does take place it is more aggressive. Schwab in his series of 164 low grade chondrosarcomas had a 13% recurrence rate and found a high rate of recurrence in those that recurred. 7 of 21 recurrences had metastases. “Recurrence may be regarded as a declaration of an aggressive phenotype and should be treated as such.”
Treat all recurrences aggressively.
References
Dahlin D. C., Cancer 1991;28:461-466
, Schwab J. H., CORR, Vol 462, 2007
Gelderblom, H; The clinical approach towards chondrosarcoma. The Oncologist 2008; 13320-329
Aarons, C.; Extended intralesional Treatment versus Resection of Low-grade Chondrosarcomas CORR, 2009, 476, 2105 - 2111