|
Video, 30 min |
Common Bone lesions appearing cystic on X ray
- Simple Bone Cyst
- Aneurysmal bone cyst
- Ganglion cyst
- Chondromyxiod Fibroma
- Eosinophyllic grannuloma
- Non ossifying fibroma
- Fibrous dysplasia
- Infection
- Hydatid cyst (fairly common in South Africa)
 |
|
| Aneurysmal bone cyst of 3rd metatarsal. Note how the other metatarsals have adapted to this slow growing lesion | |
Patients with cystic bone lesions may present with pain or swelling or the cyst may be noticed incidentally on an X Ray taken for other reasons.
Pain may indicate that the cyst is developing a stress fracture and needs urgent treatment, or it may be present for other reasons such as in the case of a ganglion cyst secondary to degenerative joint disease.
The patient commonly presents with an established fracture through a lesion that appears cystic.
 |
| Pathological fracture through a simple bone cyst in a 17 year old |
Not all cysts require treatment. In some lesions the danger of biopsy or other surgery may outweigh any benefit.
The following lesions generally do not require operative treatment.
Tumor and tumor-like lesions for non operative treatment
- Bone infarct
- Fibrous cortical defect
- Small, solitary focus of fibrous dysplasia
- Intraosseous ganglion
- Stress fracture
- Myositis ossificans
- Hyperparathyroidism - Brown Tumour
- Bone island (enostosis)
- Enchondroma in a short, tubular bone
- Avulsion fracture (healing stage)
Staging
of Benign Bone Tumours(Enneking)
|
||
| Stage 1 (latent) | Stage 2 (active) | Stage 3 (aggressive) |
| Non-ossifying fibroma Enchondroma |
Enchondroma Osteochondroma Osteoid osteoma Osteoblastoma Giant-cell tumor Chondromyxoid fibroma Fibrous dysplasia Eosinophilic granuloma Aneurysmal bone cyst Unicameral bone cyst Osteofibrous dysplasia |
Giant cell tumor Osteoblastoma Chondroblastoma Aneurysmal bone cyst |
As with everything in medicine, there are exceptions. Any lesion in the above list which is painful, fast growing or large (appears as if it may immanently cause a fracture) will require surgery.
 |
 |
| This non ossifying fibroma was so large it lead to a pathological fracture and required internal fixation | |
 |
 |
| Exceptions to the rule: Intraosseous ganglion (Gode). This lesion was painful and required a vascularised graft. | |
Management
Surgical options
- Aspiration with or without steroid infiltration
- Cyst contents aspirated and replaced with steroid infiltration
- Suitable for simple bone cyst - aspiration of blood means it is likely an ABC and recurrence likely
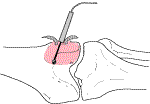
- Curettage
- Remove the roof of the cyst
- Curette contents and send for histology
- Burr the walls with a high speed burr until all tumour removed
- In lesions with a high recurrence rate (e.g. giant cell tumour) adjunctive ablation of surviving tumour cells is required
- » Cryosurgery - effective but danger to neurovascular structures and skin
- » Phenol - 80% phenol painted on inside of cyst. Wash it off with absolute alcohol after 3 minutes and irrigate thoroughly
- Cyst is filled with bone graft either autogenous or allograft.
- Block excision - reserved for expendable bones e.g. ABC in shaft of fibula. Or the higher grade lesion e.g. giant cell tumour of the proximal tibia . The whole of the involved bone is excised and the defect replaced either with an arthrodesis, or custom made prosthesis.
The stage of the tumour must be taken into consideration when treatment is planned. The protocol in the table below advocated S. Gitelis can be applied to all benign lesions, including cysts.
Treatment of benign bone lesion according
to surgical stage |
|
 |
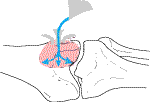 |
| After curettage the inner walls of the cyst are burred | Cryosurgery: Liquid nitrogen is poured into the cyst to ablate any surviving tumour cells |
Internal Fixation
Whether to do internal fixation or not after operating on a cyst depends on the site of the lesion. As a rule simple bone cysts do not require internal fixation and can be treated conservatively, even if they have already caused a fracture. The bone is merely treated as uncomplicated traumatic fracture, and the fact that the cyst has decompressed itself will hasten its resolution.
Any cyst in a high stress area, such as the peritrochanteric region of the femur will require open reduction and internal fixation in addition to the definitive treatment described above. Even a biopsy in this region is enough to initiate a fracture and will probably require internal fixation before the patient can be safely mobilised.
Today's Date: Sat Jul 27 02:28:17 2024
References
- (1) Enneking, W. F.:
- Musculoskeletal Tumor Surgery. Vol. 1, pp. 87-89. New York, Churchill Livingstone, 1983.
- (2) Enneking, W. F., and Gearen, P. F.:
- Fibrous dysplasia of the femoral neck. Treatment by cortical bone-grafting. J. Bone and Joint Surg., 68-A: 1415-1422, Dec. 1986.
(3) Gitelis, S., Wilkins, R., and Conrad, E. U., III- Instructional course lectures, The
American Academy of Orthopaedic
Surgeons. Benign Bone Tumours - JBJS Vol. 77-A, No. 11, November 1995, pp. 1756-1782