Fractures of the proximal femur
Most fractures through the femur neck and intratrochanteric regions occur in the elderly due to osteoporotic bone and or muscular incordination resulting in a fall. If a young patient suffers a fracture here it is often due to significant trauma and is often associated with other fractures and injuries.
The general medical condition must be assessed. These elderly patients are often dehydrated. Look out for other medical conditions, stroke and other hypertensive episodes as well as cardiac conditions may need to be diagnosed and managed.
Classification:- Extracapsular
- Intracapsular
 |
 |
Extracapsular |
Intracapsular |
Extracapsular Fractures
There is a good blood supply and these fractures will always unite. There is a tendency to union in a varus position if treated conservatively. As extra capsular fractures occur predominantly in the elderly population operative treatment is preferred to allow early mobiliastion and thus prevent the complications of bed rest.
Conservative treatment:
This is only indicated in exceptional cases such as local sepsis or the patient being too ill to operate on.
Insert a Denham pin into the proximal tibia and provide longitudinal traction 5 - 7 kg until union takes place. This may take up to 3 months.
 |
 |
Extra capsular fracture |
Sliding Screw and plate |
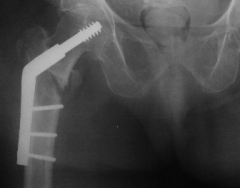
Operative treatment
The patient is operated on as soon as his medical conditions have been stabilised. A sliding screw and plate can be used. The large proximal screw can slide back in the barrel and prevent perforation of the femur head. Place the screw inferiorly in the femoral head to minimise the chances of this complication.
For unstable intratrochanteric fractures - where there is significant subtrochanteric extension or the medial buttress is compromised a intramedullary pin with screw into the femur head can be used (cephalomedullary device)
 |
 |
Unstable Extra capsular |
Cephalomedullary fixation |
After fixation the patient is mobilised as soon as possible.
Intra capsular proximal femur fractures
These fractures involve the femoral neck. They can be classified as non displaced or displaced. With displaced fractures the femur neck has moved and compromised the blood supply of the femur head.
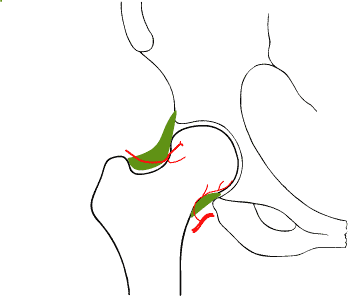 |
| Most of the blood supply of the femur head comes via retinacular branches on the femoral neck. These are damaged with displaced femoral neck fractures and there is danger of avascular necrosis |
Avascular necrosis is relatively common and may either result in non union of the fracture or in late segmental collapse, where the fracture unites, but the femoral head undergoes avascular necrosis and collapses. For this reason most displaced femoral neck fractures are operated on and the femoral head is replaced with a prosthesis.
Conservative treatment
This is rarely indicated as the femoral neck will never unite. It may be resorted to in the patient who is too debilitated for anaesthetic or gross local sepsis. The fracture is neglected and the patient is mobilised and sat in a chair as soon as possible, she is encouraged to walk as soon as the pain allows. The rationale is that the fracture will undergo pseudarthrosis and a mobile patient with a painful hip is better than death from the complications of immobilisation.
Operative treatment
This varies depending on the (physiological) age of the patient. Younger patients have can withstand possible re operation due to the complications such as non union and the femur neck can be fixed with cannulated hip screws or a sliding screw and plate. The very old get the simplest type of replacement - a Moore's hemi replacement which is un cemented. The older but relatively fit and ambulant are given a total hip replacement.
Treatment Intra capsular
Femur Fracture |
|
Age |
Treatment |
| Young (- 55yr) | Reduction and ORIF with cannulated hip screws |
| Older (55 - 75+) Fit | Total hip replacement |
| Old (>75) Unfit / Senile | Moore's hemi replacement |
The ages given in table are not absolute and indications will vary depending on the surgeon's outlook and the budget of the institution / funding available.
 |
| Moore's Prosthesis |
Social problems
A fall resulting in a hip fracture is often a life altering event. The patient often needs to be booked into an old age home. There is an appreciable mortality rate within the first two years (up to 47% in the patient with serious co morbid diseases.)