External Fixators
Department of Orthopaedic Surgery - University Stellenbosch, South Africa
| External fixation Page | |
Next Page >> |
 With external fixation, pins are inserted through the skin into the bone
and held in place by an external frame.
With external fixation, pins are inserted through the skin into the bone
and held in place by an external frame.
The usual indications are open fractures such as a tibia fracture which
requires dressings or attention to a wound or flap.
It can also be used with closed fractures e.g. unstable radius fracture.
External fixation is most successful in superficial bones e.g. tibial
shaft. Avoid it in deeper bones e.g. the femur or humerus - here the chance
of pin tract sepsis is greater.
Indications for external fixators:
External Fixators are frequently used in the management of tibial fractures.
Indications for External Fixators
- Severe open fractures / bad soft tissue damage
- Infected fractures
- Burns
- For "Damage Control Orthopaedics" (where the patient's initial condition is too critical for prolonged surgery) to provide stability, and to maintain length. The exfix is replaced by definitive fixation (pate or IM pin) once the patient stabilises. A temporary exfix can be placed over the joint for pilon or plateau fractures that are length unstable. It is later removed when ORIF is performed, once soft tissue swelling subsides (in about 10 days).
 |
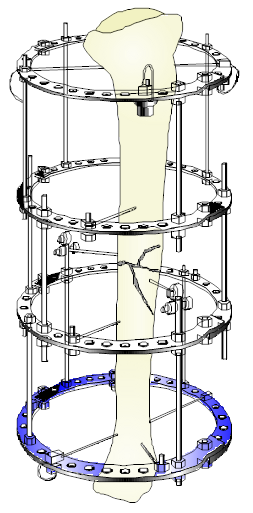
Ilizarov external fixator on a tibia. This type of fixator, although somewhat tiresome to assemble, has a low incidence of pin-site sepsis, is very stable, and is ideal in a metaphyseal region. It is often used for bone lengthening as well as bone transport procedures |
Advantages of external fixation
- The method provides rigid fixation of the bones in cases in which other forms of immobilization, for one reason or another, are inappropriate. This is most common in severe, open types II and III fractures in which cast or traction methods would not permit access for management of the soft tissue wounds and in which exposure and dissection to implant an internal fixation appliance would devitalize and contaminate larger areas and might significantly increase the risk of infection or loss of the limb itself.
- Compression, neutralization, or fixed distraction of the fracture fragments is possible with external fixation, as dictated by the fracture configuration. Uncomminuted transverse fractures can be optimally compressed, length can be maintained in comminuted fractures by pins in the major proximal and distal fragments (neutralization mode), or fixed distraction can be obtained in fractures with bone loss in one of paired bones, such as the radius or ulna, or in leg-lengthening procedures.
- The method allows direct surveillance of the limb and wound status, including wound healing, neurovascular status, viability of skin flaps, and tense muscle compartments.
- Associated treatment, for example, dressing changes, skin grafting, bone grafting, and irrigation, is possible without disturbing the fracture alignment or fixation. Rigid external fixation allows aggressive and simultaneous treatment of bone and soft tissues.
- Immediate motion of the proximal and distal joints is allowed. This aids in reduction of edema and nutrition of articular surfaces and retards capsular fibrosis, joint stiffening, muscle atrophy, and osteoporosis.
- The extremity is elevated without pressure on the posterior soft tissues. The pins and frames can be suspended by ropes from overhead frames on the bed, aiding edema resolution and relieving pressure on the posterior soft tissue part.
- Early patient mobilization is allowed. With rigid fixation the limb can be moved and positioned without fear of loss of fracture position. In stable, uncomminuted fractures early ambulation is usually possible; this may not be the case if these fractures are treated by traction or casting. Use of external fixation also allows mobilization of some patients with pelvic fractures.
- Insertion can be performed with the patient under local anesthesia, if necessary. If a patient�s general medical condition is such that use of a spinal or general anesthetic is contraindicated, the fixator can be inserted using local anesthesia, although this is not optimal.
- Rigid fixation can be used in infected, acute fractures or non union's. Rigid fixation of the bone fragments in infected fractures or in infected established non union's is a critical factor in controlling and obliterating the infection. This is rarely possible with casting or traction methods, and implantation of internal fixation devices is often ill advised. Modern external fixators in such instances can provide rigidity not afforded by other methods.
- Rigid fixation of failed, infected arthroplasties in which joint reconstruction is not possible and in which arthrodesis is desired can be achieved.
Disadvantages of external fixation
- Meticulous pin insertion technique and skin and pin tract care are required to prevent pin tract infection.
- The pin and fixator frame can be mechanically difficult to assemble by the uninitiated surgeon.
- The equipment is expensive.
- The frame can be cumbersome, and the patient may reject it for aesthetic reasons.
- Fracture through pin tracts may occur.
- It is difficult to do delicate surgery such as skin flaps once the exfix apparatus is in place. Rather do this type of surgery before the frame is applied.
- Re fracture after exfix removal may occur unless the limb is adequately protected (e.g. by walking cast application), until the underlying bone can again become accustomed to stress.
- The noncompliant patient may disturb the appliance adjustments.
- The head injured patient may injure himself by thrashing his pin studded limb against other parts.
- Joint stiffness may occur if the fracture requires that the fixator
immobilize the adjacent joint. e.g. an exfix placed over the ankle for
a pilon fracture as there was insufficient space for pins in the distal
tibial fragment.
Complications
There are many potential complications with sepsis being the most common.
Pin tract infection. Without proper technique for pin insertion
and meticulous pin tract care, this may be the most common complication,
occurring in 30% of patients. It varies from minor inflammation remedied
by local wound care, to superficial infection requiring antibiotics, local
wound care, and occasional pin removal, to osteomyelitis requiring sequestrectomy.
A "ring sequestrum" is the radiological appearance of a sclerotic
ring about the hole left from a transfixion pin (from an exfix or other
skeletal traction device.
Neurovascular impalement. Know the anatomy of the underlying limb,
and avoid major neurovascular structures. The surgeon must be familiar
with the cross-sectional anatomy of the limb and with the relatively safe
zones and danger zones for pin insertion The radial nerve in the distal
half of the arm and proximal half of the forearm, the dorsal sensory radial
nerve just above the wrist, and the anterior tibial artery and deep peroneal
nerve at the junction of the third and fourth quarters of the leg are
the structures most often involved. Vessel penetration, thrombosis, late
erosion, arteriovenous fistulas, and the formation of aneurysms have also
been observed.
Muscle or tendon impalement. Pins inserted through tendons or muscle
bellies restrain the muscle from its normal excursion and can lead to
tendon rupture, or muscle fibrosis. Ankle stiffness is frequent if multiple
transfixing pins are used in fractures of the tibia.
Delayed union. The rigid pins and frames can ��unload�� the fracture
site, with cancellization and weakening of the cortex similar to that
noted with internal rigid compression plate fixation if the fixator remains
in place for several weeks or months. The callus produced is entirely
endosteal, and delayed unions in 20% to 30% (and as many as 80%) of fractures
have been reported in the literature with prolonged use of the rigid fixator.
Compartment syndrome May occur in the limb treated with an external
fixator. Unlike open surgery which opens facial planes, an external fixator
is basically a closed method and there is a higher rate of compartmental
syndrome.
Refracture. Union due to the rigid fixation is largely endosteal,
with very little peripheral callus formation. The de stressing of the
cortical bone by the rigid fixation results in cancellization of the cortex;
refracture is possible after fixator removal unless the limb is adequately
protected by crutches, supplemental casts, or supports.
Limitation of future alternatives. Such methods as open reduction become
difficult or impossible if pin tracts become infected. If an external
fixator is left in more than a week, there is a higher rate of infection
if open reduction and internal fixation (ORIF) is later attempted. Do
not use an exfix for an extended period ,if you anticipate open reduction
will later be required. It is safe to do ORIF, however if the exfix removed
within a week of application. In "Damage Control" surgery i.e.
where anaesthetic time must be limited due to other life threatening conditions,
in the multiply injured, a temporary exfix is a solution. Later when the
patients condition stabilises, the exfix can be replaced by performing
definitive open reduction and internal fixation.
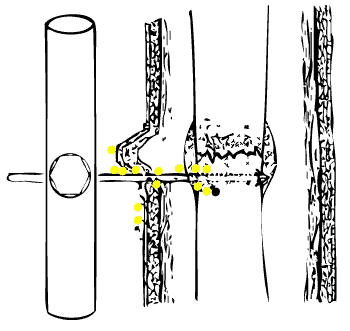 |
Avoid causing osteomyelitis Skin "tenting" i.e. folds caused by skin compression against the pin must not be tolerated - these folds lead to pin tract sepsis. Make a relaxing incision on the side of the fold, and suture any resulting wound. |
Causes of pin sepsis
- Site selection
- The more soft tissue there is, the greater is the chance for sepsis. Site the pin where the bone is as superficial as possible.
- Skin tethering
- Place the pin so as not to tension the skin. Close wounds, if possible before inserting the pin, as closure will be likely to move the skin. Make relaxing incisions to relieve skin tension - suture the resulting defect if necessary.
- Use of power instruments
- Drilling wide diameter pins directly into bone will generate heat, this may lead to sequestrum formation and sepsis. Either pre drill the pins with a helical drill, or use hand instruments to insert the pin.
- Pin Care
- Inadequate pin care and poor hygiene may lead to sepsis
Pin Care
- Clean the skin / pin interface of all discharges twice daily
- Antiseptic dressings - "Betadine" (povidone) ointment
- Inflamed or septic skin about a pin (not loose) - Appropriate (oral) antibiotic
- Septic Loose Pin - remove, and replace with another through normal skin
- Simple outpatient procedure
- Remove the exfix once its job is done. Replace the device with POP cast once skin defect ( the reason the exfix was put on for) has healed, and fracture has stabilised enough not to easily displace.