|
Differences between benign and malignant tumoursBenign tumors are unable to metastasize and generally grow slowly.
|
Simple bone cyst This is a common
bone tumor in children and may lead to pathological fractures. If it
is painful, the cause is usually mechanical stress ( pre fracture stage)
and symptomatic lesions should be treated.
This is a common
bone tumor in children and may lead to pathological fractures. If it
is painful, the cause is usually mechanical stress ( pre fracture stage)
and symptomatic lesions should be treated.
 Cysts in the region of the hip are particularly prone to fracture.
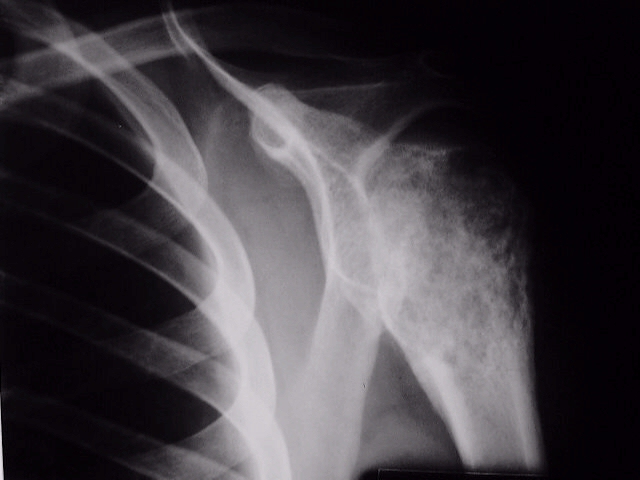
TreatmentSymptomatic or cysts in high stress areas such as the femur neck need treatment The cyst needs to be decompressed. Methods such as curettage and bone graft, injection with cortisone and simple drilling with K wires are all effective. Fractures through a cyst are treated conservatively ( plaster cast). In high stress areas such as the hip, internal fixation is needed. The cyst usually resolves after the fracture unites.If a cyst recurs a biopsy is needed, as the diagnosis may be a more aggressive entity such as the aneurismal bone cyst. Aneurysmal Bone CystIs a cystic expansile bone tumor seen in the first and second decades. It may appear in any bone.
 primary lesion such as a GCT, chondroblastoma, fibrous dysplasia, chondro myxoid fibroma, EG, simple cyst, osteoblastoma, non ossifying fibroma The ABC can become large, and can also be the cause of a pathological fracture. Some ABC 's can be fast growing and locally aggressive. Biopsy and histological diagnosis is mandatory if ABC is suspected. Treatment is by curettage and packing with bone chips.
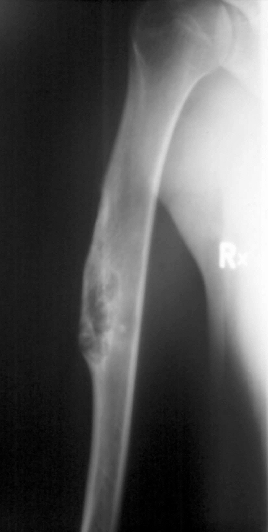
EnchondromaA benign cartilaginous lesion appearing in adult life, seen often in short tubular bones e.g. the hand. The lesions are usually single but may be multiple.
X-rays show scalloped erosions on endosteal surface. There may be flecks of calcification. In multiple enchondromatosis (Ollier's disease) there may be associated deformities, such as genu varus or valgus. In the systemic form (Ollier's), there is a high (10 -20%) incidence of malignant transformation.
Treatment is by curettage and bone grafting. Because many of these may be low grade malignant chondrosarcoma ( which is difficult to distinguish histologically from benign enchondroma) additional techniques, such as cryosurgery are also added to make sure the residual cells are killed.
|


Non Ossifying Fibroma
 primary lesion such as a GCT, chondroblastoma, fibrous dysplasia, asymptomatic and found incidentally on X-rays Large lesions may cause a pathological fracture. Treatment is only required in a symptomatic lesion. The defect is curetted and packed with bone.  If
found incidentally on x rays and the lesion is small, leave it alone.
Larger lesions are rare, but if > 50% of diameter of the bone consider
surgery, as pathological fractures can take place. If
found incidentally on x rays and the lesion is small, leave it alone.
Larger lesions are rare, but if > 50% of diameter of the bone consider
surgery, as pathological fractures can take place. |

Fibrous dysplasiaHistologically also fibrous tissue. Is a more severe and often systemic form non os sifying
fibroma. It begins in childhood and affects one (monostotic) or many
bones. It may cause deformities such as coxa vara and facial deformities. sifying
fibroma. It begins in childhood and affects one (monostotic) or many
bones. It may cause deformities such as coxa vara and facial deformities.X-ray features Radio lucent or opaque lesions may be lobular or scalloped. The cortex is eroded and expanded. |
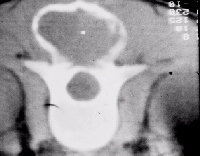
Osteoid OsteomaOsteoid osteoma presents as a sclerotic cortical lesion. It is painful and the pain is relieved by asprinThere is an oval lytic centre known as the nidus. It is this center that produces benign osteoid.
Management To locate the nidus computer tomogrammes are helpful. A technetium scan will show a hot spot. Excision of the nidus will cure the pain. An en block excision is done. |

OsteochondromaThe osteochondroma is common and presents as a bony outgrowth near an epiphysis.
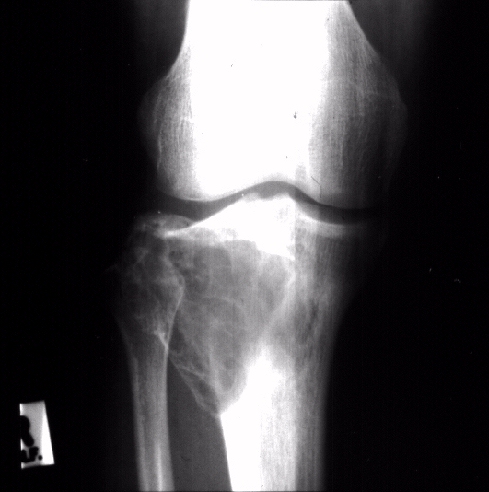
Management Not all lesions require excision. Excise symptomatic lesions and do histology. In multiple osteochondroatosis yearly technetium scans are done and hot lesions are excised. All symptomatic lesions must be excised. Giant Cell TumoursThe Giant Cell Tumor grows in the epiphysis of adults and undermines the mechanical integrity of the joint.
Treatment The GCT consists of giant cells in a spindle cell stroma. The often breaks through the bone and invades the soft tissue.  primary lesion such as a GCT, chondroblastoma, fibrous dysplasia, On rare occasions it metastasizes to the lungs. The tumor is curetted and packed with bone. This may fail if it is a major joint and block excision may be required with arthrodesis or joint replacement. ChondroblastomaThe chondroblastoma has a predilection for the epiphysis and is almost always found here. It does not stretch to the articular surface as the GCT does.
 primary lesion such as a GCT, chondroblastoma, fibrous dysplasia, Treatment Curettage and bone graft. Chondromyxiod FibromaThe Chondromyxoid Fibroma is composed of myxoid or primitive cartilage and fibrous tissue. It presents in the second decade or later.
 primary lesion such as a GCT, chondroblastoma, fibrous dysplasia, Treatment Extra capsular marginal excision. Recurrence is rare. |